Want to make sure you keep in touch with the MSPress Blog and upcoming MSPress Journal? Follow us on Facebook and on Twitter! Want to communicate with us? Email editorinchief@themspress.org or use #themspress in your posts!
I am a medical student because I love questions. After a blood vessel takes a punch, what causes the platelet pile-up? What makes people blink, gag, cough, or sneeze? Why is cat litter as scary as alcohol for a pregnant woman?
Some medical questions are unanswered. Yet, science promises progress. With enough grant-funded work in labs and clinics, scientists can describe new diseases. Medicine will show where illness happens, researchers will explain how it happens, and epidemiologists will predict who it is more likely to happen to and when it could happen to them. Even with all of this knowledge, there is one question I do not expect my medical training to answer.
While I go to lectures, practice interview skills, and learn how to diagnose and prescribe, people endure pain, distress, and loss, and I can’t explain why. Why do people suffer?
I can look to people who suffer for answers. It is not hard to find written first-person narratives of suffering. In these narratives, protagonists are often cast in two roles: the suffering fighter and the wise sufferer.
As Kathlyn Conway discusses in her essay, “The Cultural Story of Triumph”, the narrative of a “suffering” fighter dominates over other stories of illness. Illness becomes a journey to physical cure. Where physical cure is not possible, illness is cast as a path to wisdom, a form of moral development. The patient becomes a traveler who should somehow be “uncomplaining, strong, and brave” on this journey (Conway, 2007).
“Illness is a chance to show us your guns and triumph!” the medical culture seems to say.
If society expects sick people to be “fighters” what else do we expect from them? I think of S, a 62-year old woman with osteosarcoma, who put on lipstick while her skin was sinking deeper into the spaces between her bones. “Can’t let this cancer make me ugly honey,” she said as she applied her makeup in the mirror. What does it mean that S’s fight against cancer involved cosmetic routines?
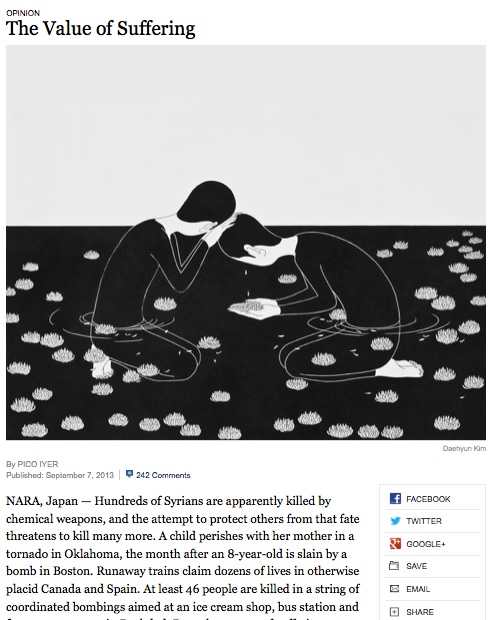
The idea that people grow in strength or wisdom while suffering is familiar to me. As essayist, Pico Iyer describes in “The Value of Suffering”, suffering can be a doorway to compassion, loss can be an invitation to appreciate nuance. Yet, my intestines tangle when I imagine telling a patient who suffers, “What an opportunity to unfurl in wisdom!” Even if I did not say this out loud, I wonder what my expectations might communicate.
Last year, my close friend J died of metastatic breast cancer while 27 weeks pregnant with a boy. During her first trimester, we would lie on my floor and look up at the ceiling when retching woke her in the morning. Over the next few months we went to her prenatal visits and giggled over possible baby names. Then, she stopped eating and her nails turned yellow. Her doctor said, “Hopefully it’s hepatitis.” He didn’t bother to tell us what it hopefully wasn’t. Her yellow vomit and “liver nodules” explained. She was 24 years old when she passed away and left behind her husband and 3-year old son.
That was an inexplicable catastrophe. But J’s husband needed to believe that somehow God had planned this. If he believed that her death was one example of many forces that roll over us the way tires would ants trying to cross a highway, then how could he continue with day-to-day life? How would he keep being his son’s Papa?
Even after I gather years of experience with suffering, I do not expect to be able to explain it. I do know that the stories we tell about suffering can influence how we relate to patients.
My expectations form the questions I ask and the things I attend to. Imagine me telling a patient, “Fight your cancer, but stay pretty. Also, grow spiritually so you can teach me through your suffering.” That feels like a lot of pressure to put on someone who is ill, even if it is unspoken. If I look for a suffering fighter in a patient who cannot cast herself in that role, I risk disrespecting her experience. If I try to learn wisdom from a patient who does not see his illness as a journey to moral development, I might disregard his life story.
Medical school teaches me to synthesize and simplify information. The more narratives I hear, the more I feel a desire to string them together along a unifying theme. Cultivating attention to less common stories about suffering and loss reminds me to listen when I long to explain.
Sources:
Conway, Kathlyn. 2007. Beyond Words: Illness and the Limits of Expression. University of New Mexico Press. Albuquerque
Iyer, Pico. 2013. The Value of Suffering. New York Times. Featured image:
“After a Night Shift” by Stephanie Scott
The day’s clinical case presented in anatomy lab was that of a 40-year-old male who had dislocated his sixth cervical vertebrae in a surfing accident. Upon arrival at the hospital, he had suffered full paralysis from the neck down but was still conscious and alert. He and his wife were told that surgery would be needed to repair his broken neck, but that the chances were very slim that he would ever regain the functions he had lost due to the injury. The last page of the case was an X-ray image of the man’s vertebrae fused with screws and plates realigning his spinal cord. His prognosis was left to the students’ speculation. We returned to the classroom to debrief the case.
As a group, we discussed the grim injury in all of its anatomic and physiologic glory. Guest surgeons explained the gravity of the man’s situation and the devastating symptoms with which he presented. The case ended as they all do: we hoped for the best for our fictional patient but understood the assumed permanence of an injury of this type.
There was a long pause before Dr. Payer said, “Would you like to meet him?”
Shocked, we all turned to the back of the room where Dr. Topping was opening the door for our patient – would he be in an electric wheelchair? Would his body appear atrophied and weak from years of paralysis? How would he get down the steps in our classroom?
A strong, unfamiliar voice echoed from the front of the classroom. “Hi, everyone.”
We turned around to see who could be distracting us from seeing our patient come through the door. It did not take long for us to all realize that the man standing before us on two perfectly healthy legs, holding a microphone with two fully-functioning hands, with zero sign of ever having suffered a devastating cervical subluxation, was our patient. All 120 of us gasped in unison. It was an incredible sight, an absolute medical miracle. When you spend your days studying everything that goes wrong with the human body, it is amazing to see something that went right−the experience had me in tears.
He filled in all the gaps of the case and explained the details of his injury and his recovery. He talked about his physicians and surgeons and how he had ran the Turkey Trot just two months after his accident. Then, his best friend who happened to be a physician at the hospital to which he was flown told us the most important factor in his return to normalcy: when everyone else had lost hope, he never did. He refused to accept a prognosis of permanent paralysis. He refused to accept the possibility of an unsuccessful surgery. He never gave up on his body, so his body never gave up on him.
This story is, of course, rare. And yet, it speaks volumes about the power of the human spirit. As a medical student, I will be one of the last people to refuse credit to the nurses, physicians, paramedics, and surgeons who undeniably saved this man’s sense of a normal life. But I also know firsthand what happens when you give up. Keeping hope does not mean you automatically win the battle. But the alternative guarantees a loss.
It is a concept that I have been battling with since I began medical school. As a pre-medical undergraduate student, I had nothing but the utmost confidence in myself. I saw myself receiving my white coat. I saw myself as a doctor. Of course, I had my doubts – especially around application season. But even on my darkest days, I knew I could get to medical school. I made it, and in the process, have lost all confidence in myself. I feel as though I am the only one who does not believe in my ability to succeed. I feel like a fake, an imposter; as though I’m floating through a movie scene just waiting for someone to yell “CUT!” Perhaps it is because the next step is actually being a doctor. The next step no longer involves passing a module exam and meeting research deadlines. The next step involves real people, real families, real life, and real death.
And yet, I could not feel more at home. There is really no place else I would rather be. But I still fall asleep every night to a lullaby of forced distraction as my mind tries to convince me that I cannot do it, that I will not make it through, and that everyone else has such a better handle on life than do I. And once you lose hope, no amount of distraction can help you fall asleep. Give up on your mind, and it will give up on you.
I recently had the privilege of visiting The Seedfolk Store in Rochester, New York. The store is run by the non-profit ProperRochester, Inc. which focuses on community engagement through urban agriculture with a focus on healthy food availability, youth empowerment, and entrepreneurship. The shop takes some inspiration from the book “Seedfolks”, a children’s novel by Paul Fleishman, in which an ethnically diverse community in Ohio works together to transform a vacant lot into a garden. I visited the shop as part of an activity for a medical humanities course I am currently taking, entitled “Death by Zip Code”, taught by Katrina Korfmacher, Ph. D. This course explores the importance of the environment on population health, focusing on epidemiology. The Seedfolk Store provides some vegetation in an area that is otherwise a “food desert”. These areas usually have fast food restaurants and convenience stores/corner shops. The Seedfolk Store has a refrigerator full of vegetables that are often requested in the area by neighbors. As a new organization, they are working on spreading the word about their efforts and services. While a full-fledged vegetable market would be unsustainable and unprofitable, this hybrid-shop is a great compromise and is catered to current demand. The shop gains some profits by selling granola from Small World Bakery, selling coffee for Coffee Connection, and selling potted plants and green tea bags that they make.
The staff’s experiences with ProsperRochester, Inc. is inspiring−it is clear to me that this team is daring and ambitious. They are dedicated to teaching youth about the specifics of food planning, processing, and distribution (selling and educating). These youth are employees and volunteers who work at the Seedfolk Store, green house, and in community gardens. They are actively involved with cooking education, small-scale food production, urban farming and learning about the local food system. The Seedfolk Store provides nutrition workshops, cooking classes, soup for the general public on Tuesdays, potted plant sales at the Rochester Public Market, and a rentable kitchen space for cooks. On April 12th, the team began planting at the M.K. Gandhi Institute for Nonviolence, a community partner which provides ProsperRochester, Inc. with space to widen in-ground gardening. In many locations, ProsperRochester, Inc.’s concerns about lead in soil has led to their use of raised bed gardening. ProsperRochester, Inc. also works closely with In the City Off the Grid, with which they are creating an aquaponics agriculture system at the Gandhi Institute and expanding a hydroponic greenhouse on Rochester’s East Main Street.
Most inspiring is that The SeedFolk Store’s team truly lives the message of health that they promote. Three members lost large amounts of weight and they told us their secret−namely they changed their diet, eliminating refined grains and processed sugars while increasing their intake of fruits and vegetables. One of the cooks renting the kitchen is a cheerful immigrant from Africa who wrote a children’s book about nutrition. She brought her own cooking supplies to The Seedfolk Store’s kitchen and waited in the rain for her ride home. This determination to further the health of one’s community through nutrition, no matter the obstacles, is very much necessary in all urban areas in the United States. I hope to help spread the word about this initiative and soon see similar projects pop up across the country to empower youth with the ability to make healthy life choices.
To visit The Seedfolk Store online or in person: The Seedfolk Store 540 West Main Street, Rochester, NY, 14611 (585) 279-9943
Entering the first year of medical school, MS1’s believe that they have some idea of what they are beginning. We are inundated with information about medical school starting in our pre-med or post-baccalaureate years, and the application process heaps even more onto our plates. Along with this, we have stories passed down by older friends and relatives who have already started or gone through the medical school experience. When we finally get to school, we think nothing will surprise us.
Needless to say, this naiveté is quickly shed after the first week of classes. We soon realize that we have much to learn, and very little time to learn it in. Some of these lessons occur in the classroom, while others remain more personal. After having gone through most of my first year, I have some surprising lessons.
Here’s my Top 5:
1. The amount of material you learn in a short period of time is amazing.
I was an immunology major in college. I took two semesters of lecture and one semester of lab to qualify for this major, on top of all of the other pre-med requirements. My immunology course in medical school was three weeks long. The medical school course covered more materialthan my core undergraduate major classes in 27 fewer weeks.
You learn so much in medical school so quickly that it is at times mind-boggling. While you do adjust somewhat to the coursework, you will still be amazed at how much you are expected to know from every day of class. Some people deal with this by studying all day, while others procrastinate and spend the days leading up to the exam stress eating pounds of chocolate. Either way, you get through it and come out more knowledgeable (and slightly heavier) than before.
2. Medicine has its own language, and it makes no sense at all.
Nothing, absolutely nothing, is put into layman’s terms. You can’t say “elevated heart rate”, you must say “tachycardia.” You can’t say “shortness of breath”, you must say “dyspnea.” You can’t say “low platelets,” you must say “thrombocytopenia.” That last one is my personal favorite. The ridiculous nature of this system is apparent to everyone, but since it’s been entrenched in the medical community for so long, it continues onwards. Have fun, future medical students.
3. You become desensitized to gross masses/fluids/images.
Menstrual fluid? No big deal. Oozing pus from a skin lesion? Not interesting. Penile sischarge? Just another Tuesday in the infectious disease/STD clinic. Teratoma? Well, that one is still rough. If you haven’t seen a teratoma, I’d suggest you google it (not at work, definitely NSFW).
4. Everyone is smarter than you.
I’m amazed every day by all of my classmates. They are all so accomplished and humble. One of my classmates is a published author (of a real book, not a research publication). One is a pilot. Another, an investment banker before beginning medical school. My college days of playing too much Xbox Live, while impressive for sheer immaturity, pale in comparison.
What I’ve really come to realize, however, is that you can learn a lot from viewing how others reach success. I’ve picked up many good habits and behaviors by just observing how my accomplished classmates go about their lives. As they say, imitation is the sincerest form of flattery.
5. Medical school is truly life changing.
For how much everyone complains about medical school, no one can deny that it is life changing. You learn so many interesting things, and all of them are relevant in positively affecting the lives of others. You meet so many interesting classmates and mentors, forming a motivating and comforting community. Most importantly, medical school teaches you about yourself. You learn that you are capable of so much more than you previously thought, and that you can deal with any challenge. All of these lessons and experiences are, quite literally, worth the price of admission.
Photo courtesy of https://www.flickr.com/photos/zsoolt/
The Croatian constitutional court has made the vaccination of children a legal obligation. Their reasoning behind this law is that “a child’s right to health is more important than a parent’s right to choose (wrongly)”. Their words, not mine, although I do agree.
Vaccination has been a part of paediatric care in Croatia for years, and children have regularly been vaccinated throughout their education, although it has never before been officially mandatory. Now, parents have the potential of being prosecuted if they do not to vaccinate their children. In Croatia, children are vaccinated against the following: tuberculosis, diphtheria, tetanus, pertussis (DTaP), polio, measles, mumps, rubella (MMR), and hepatitis B. It was always said that vaccination was mandatory, but whenever I asked what to do with unvaccinated children, I was given vague answers. Nevertheless, the law now states that a parent’s failure to ensure the vaccination of their child will result in a fine and a visit from social services. A large group of parents, accompanied with some medical professionals, disagree with this and have called for a public discussion.
This is an argument many parents have repeated when asked why they don’t want their children vaccinated. The majority of “modern” parents are best pals with Doctor Google, who has told them stories about apparently unnerving side effects of certain vaccinations. Furthermore, media dramatization and sensationalism add another factor in the vaccine debate. Although the Internet and media in general can provide strong patient education, it can also provide highly biased information thereby providing harmfully improper patient education. Even though they are dramatic and stand out, articles reporting on a child developing a long term and/or life changing disorder or condition are quite rare. Reading such an article invokes fear in readers. Statistics are what matter in possible negative outcomes. How many stories about serious problems arising from a vaccinations exist? And how many children are vaccinated every day? And what are measles, mumps, rubella, polio, pertussis, and the other diseases like when they take hold of a child’s body?
Understandably, parents want to protect their children and don’t want their little ones to suffer any life changing side effects, short or long term. Before allowing for any vaccination, they want doctors to tell them with absolute certainty that no harm will come to their children from a vaccine. Surely parents would also like completely safe transport, but they are willing to put their children in a car, train, or plane because of the benefits of fast travel outweigh the small chance of an accident happening. It is impossible to expect doctors to claim that anything is completely safe, and “take responsibility“ if anything at all goes wrong. This is why there are patient consent forms and small directions in all medication boxes explaining possible side effects. If a parent asked me whether I would take responsibility for any possible side effects of vaccination, I would reply with another question: Would you, as a parent, take the responsibility of your child getting an infectious disease that could leave them with life changing consequences, or even possibly be a cause of death?
Although I would try and talk to people who refuse vaccination, if they continued to refuse I would respect their decision. In the end, I appreciate it is your right to decide what you want to do with your body. A friend of mine has pointed out to me that this law might limit the right of choice; therefore not allowing parents to make a choice about their children. I can see his point, and as I said, everyone should have the right to decide what to do with their body. However, this is a choice parents aren’t making about themselves, but about their children, who are too young to make an informed choice. Are their parents making an informed choice though? Do they have enough information to go against medical advice? Many countries don’t have a law about mandatory vaccination, and maybe those fighting against this law will manage to win, but I hope this whole debate will at least raise awareness and make people think about the importance of vaccination.
Photo courtesy of Moyan Brenn https://www.flickr.com/photos/aigle_dore/
Informed Consent, written by Deborah Zoe Laufer and directed by Sean Daniels, aims to show the emotional, psychological, and physical dangers that can occur when researchers fail to communicate adequately with their subjects. The play focuses on the tale of the Havasupai tribe and their battle against the improper use of their blood in genetics research. Laufer has stated she was inspired to chronicle their story after reading a New York Times article from 2010 entitled, “Where’d You Go with My DNA?”1The article summarizes the plight of the Havasupai, a Native American tribe plagued with type II diabetes mellitus. The tribe looked to researchers at Arizona State University to study blood samples of tribal members in an attempt to find a genetic link for the disease. Of note, is that blood is sacred to the Havasupai and they will not proceed to their desired after life without their blood. Though they believed to only consenting to diabetes research, the informed consent document was “intentionally vague” and researchers decided to use the blood sample for more studies than diabetes, without re-informing the Havasupai. It is this story that lead Laufer to her play, Informed Consent. Though inspired by true events, Laufer chose to fictionalize many aspects, while maintaining the central issue: What constitutes informed consent? On March 18th, the play made its world premiere at the Geva Theatre in Rochester, New York and will be playing through to April 13th. It will be then featured in the Cleveland Playhouse in Cleveland, Ohio from April 23rd until May 18th.
This character driven play features five actors, each jumping into different roles throughout the show. Their impeccable performance is matched by a beautifully rendered set design. Created primarily of cardboard, the set aims to depict the base of the Grand Canyon−the home of the Havasupai. In contrast to the sand colored canyon, there are white rectangles scattered throughout the set, juxtaposing nature with the sterility of the science research lab. While the actors’ performances are strong in conveying the strife endured by the Havasupai, there are occasional parts that take away from the brevity of the content. This is seen with random background interjections from actors not involved in certain scenes. It seems as though Laufer attempts to add comic relief to the script; however, it is misplaced and hardly receives any laughs from the audience. Lightheartedness is out of place when addressing such a sensitive topic based on true events.
Of note is the lead female protagonist, Gillian, who conducts the research with the Havasupai. It is because of her ill-guided decision to use the blood obtained from the Havasupai for more than diabetes research, which is all that the tribe agreed to, that she inflicts pain on a tradition-dependent group. She is painted as self-centered and career driven, allowing nothing to stand in her way to get publications in lofty journals such as Nature and Cell. She goes so far as to publicly deny the creation story of the Havasupai, which the tribe has passed down for hundreds of year.
While some may think Gillian is over caricaturized, it is easy to see parallels in the everyday medical world. It’s the doctor who asks for a urine sample without telling the patient what he is testing for. It’s oversimplifying or leaving out details because a doctor thinks it is “best for the patient.” I even saw this in myself on the night of the show. After the play, there was a “talk-back” session featuring the director, a clinical geneticist, and a Native American man, not from the Havasupai tribe. When asked about DNA, the Native American man stated that he was “skeptical” of DNA and that he did not place much trust in its usage. I nearly jumped out of my chair. How could one not “believe” in something with such tangible proof? In that instant, I was Gillian, the overzealous scientist with tunnel vision whose sole perspective is scientific. Though momentarily shocked, I was pleased with this experience for play aims to make individuals realize the importance of respecting differences in opinions and beliefs. It will be through the understanding of patients’ perspectives throughout our careers as physicians that we will gain insight into their lives and, hopefully, provide them with the best personalized care we can offer.
For a medical student, anatomy lab is a rite of passage.
Everything about it is a test: Can you withstand the sharp sting of formaldehyde at 8 AM? Can you differentiate between the vagus and the phrenic nerves? Can you delicately dissect the muscles of the forearm?
Can you make that first cut?
Human emotion fascinates me and my psyche just so happens to be a complex, peculiar, and interesting specimen to study. The psychological effects of working in the anatomy lab had a profound impact on me, even with scalpel in hand two months after my first day. Day one of lab went just as I had anticipated: I kept my cool until someone broke my composure by casually asking how I was doing. I fought back tears after the harmless inquiry until I could isolate myself and let it all out in a corner between a large window and a countertop covered in plastic model brains. I had been trying to make a positive first impression on my lab group by keeping a composed demeanor despite being in an environment worthy of vast displays of emotion. Clearly, this was no simple task. Although mixed with a bit of embarrassment, I immediately felt relief upon the crumbling of the emotional dam that I had worked so hard to build. I would have stayed in the corner longer to release all of the fear, sadness, and confusion had I not felt so guilty about leaving my group within the first five minutes of lab. I typically use distraction techniques to rid myself of negative thoughts but the impending return to the lab table invalidated those tricks. Instead, I accepted that I had nothing to be embarrassed about, that I could sort through my feelings on my bike ride home, and that it is okay to let my classmates see me cry. One deep, cleansing breath later, I rejoined my group and together we embarked on our seventeen-week journey.
After that episode, I dreaded returning to the chilled tank that housed the body of a woman who could have been my mother: same age, same surgical scars, same body type. In the seven-day interim, I pondered her life. I wondered about her family, where she had worked, what made her choose to donate her body. I wondered if she died in peace or in pain. I thought about the people in my life who had passed away. Each of their deaths was sudden, painful, unanticipated, and unjustified, and left me with an incredibly significant sadness. I wondered if my perspective on death was natural, if it was normal for me to feel such heartache in the presence of a deceased stranger. I eventually concluded that there is no perfect answer because there is no norm by which to judge my perspective. With that understanding, I made peace with my emotions.
My sadness subsided over the subsequent weeks as I found myself head-over-heels in amazement and respect for the human body. I felt like a pilgrim finally reaching a sought-after shrine, seeing for the first time with my own eyes the conglomerate of vessels, nerves, organs, and muscles that until then I had only ever read about. Despite the body’s collective complexity, the individual parts seemed unbelievably simple and incapable of carrying out the multitude of physiological functions required for life.
As we uncovered one pathologic finding after another in our hunt to determine our cadaver’s cause of death, I began to involuntarily formulate a mental scenario of this woman’s final years, months, and even the day she died. Soon enough, each physical finding that suggested a potential cause of her death was accompanied by an imagined reproduction of her life. One half of me was determined and anxious to uncover new pathology that might lead to a stronger differential and the other half wished it could painlessly declare natural causes. In the histology lab, I encountered yet another emotional challenge. One minute I was eagerly anticipating visible signs of liver metastasis and the next I was welling up behind the eyepiece of my microscope, imagining our young patient receiving the news that she had five months to live.
No two medical students have the same anatomy lab experience. For me, the past nine weeks have altered my view of death and further sensitized me to human suffering. Death no longer seems personal, but rather a fundamental biologic process. It is the suffering that often precedes death that has consumed me as an anatomy student. Death undoubtedly brings about a suffering all its own—which was my initial source of heartache at the beginning of lab season. Who did this woman leave behind? Are they still grieving over her passing? But as we uncovered her countless medical problems, I wondered what was harder for her family and friends: to live with her absence, or to live with her suffering?
When it comes to anatomy lab, many medical students would express that there is nothing to it — it is simply another requirement. For others, it is unashamedly so much more. It is said that the cadaver is the medical student’s first patient. I only wish I had the opportunity to thank mine.
Featured photo courtesy of UC Davis School of Medicine