Telehealth has rapidly evolved from a supplementary healthcare service into a vital component of the modern healthcare system. Spurred by the COVID-19 pandemic, its adoption has skyrocketed, offering a glimpse into a future where healthcare is more accessible, efficient, and patient-centered. This article explores the profound impact of telehealth on expanding access to care, improving cost-effectiveness, and the challenges that remain for its widespread implementation.
Expanding Access to Care:
Telehealth’s most significant advantage lies in its ability to extend healthcare access to populations previously underserved. For rural communities, where access to specialized care is often limited, telehealth has marked improvements in health outcomes. A 2021 study published in The Journal of Rural Health found that telehealth reduced the need for travel to urban centers for specialist consultations by approximately 30%, bridging the gap in healthcare access for rural populations. Additionally, telehealth has been particularly beneficial for individuals with mobility challenges and chronic conditions.
For example, a study by Doraiswamy et al. (2022) highlighted a 30% increase in healthcare utilization among patients with mobility impairments, leading to better management of chronic conditions such as diabetes and COPD. Furthermore, telehealth’s convenience has significantly increased patient adherence to treatment plans. During the COVID-19 pandemic, the American Medical Association reported a 35% increase in telehealth visits for chronic disease management, underscoring its role in enhancing long-term health management and improving overall patient outcomes. These examples demonstrate how telehealth effectively bridges access gaps, supports diverse patient needs, and fosters improved health outcomes across various populations.
Cost-Effectiveness and Efficiency:
Telehealth is not only improving access but also contributing to cost savings within the healthcare system. By reducing the need for in-person visits, telehealth decreases transportation costs, time off work, and other associated expenses. Additionally, telehealth can help to alleviate the burden on emergency services by offering an alternative for non-emergency consultations, leading to a more efficient allocation of healthcare resources.
A 2022 study published in Health Affairs estimated that telehealth could save the U.S. healthcare system over $10 billion annually. These savings are primarily attributed to the reduction in unnecessary hospital visits and the optimization of care delivery processes. As healthcare costs continue to rise, telehealth presents a viable solution for enhancing efficiency while maintaining high-quality care.
Challenges and Considerations:
Despite its many benefits, telehealth faces challenges that must be addressed to ensure equitable access. The digital divide, characterized by disparities in access to technology and reliable internet, poses a significant barrier to widespread telehealth adoption. Low-income households, elderly populations, and those in remote areas are particularly vulnerable to this divide, limiting their ability to benefit from telehealth services.
Regulatory and reimbursement challenges also hinder the full integration of telehealth into the healthcare system. While the pandemic prompted temporary regulatory relaxations, permanent solutions are needed to sustain telehealth’s growth. Policymakers are currently working to streamline these regulations and improve reimbursement policies, but continued efforts are essential for long-term success.
Conclusion:
Telehealth represents a transformative shift in healthcare, with the potential to make care more accessible, cost-effective, and patient-centered. As the evidence in favor of telehealth continues to grow, it is imperative that healthcare systems and policymakers work together to address the challenges and fully integrate telehealth into the continuum of care. By doing so, we can ensure that the progress made during the pandemic is not just temporary but forms the foundation of a more resilient and equitable healthcare system.
Bio:
Dipti Shah holds a master’s in physical therapy and has over 10 years of experience in the field. She is passionate about integrating innovative healthcare solutions, such as telehealth, to improve patient outcomes and accessibility. Dipti’s insights are informed by her extensive clinical experience and commitment to advancing modern healthcare practices.
References:
The Journal of Rural Health. “Telehealth’s Role in Rural Healthcare Access.” 2021.
American Medical Association. “The Rise of Telehealth During the COVID-19 Pandemic.” 2021.
Health Affairs. “Telehealth and Its Potential for Cost Savings in U.S. Healthcare.” 2022.
American Telemedicine Association. “Policy and Regulatory Considerations for Telehealth.” 2023.
The Nielsen Company. “The Role of Telehealth in the Modern Healthcare Landscape.” 2022.
By: Sanjana Reddy, Tsola Efejuku, and Courtney Holbrook
In the seminal 2006 text, Redefining Health Care, Harvard Business School professors Michael Porter and Elizabeth Teisberg describe a healthcare market with a “positive sum” game; a market where all professional and economic incentives are aligned towards the maximization of “value,” defined as the “the quality of patient outcomes relative to the dollars expended.”1 Value in health care is the measured improvement in a patient’s health outcomes for the cost of achieving that improvement.1 Value-based care transformation is often conflated with cost reduction methods, quality improvement, or even evidence-based care guidelines. Rather, the goal of value-based care is to enable healthcare systems to improve health outcomes for patients over the full cycle of care. Tiesberg further elucidates three key dimensions (the Triple C’s) for measuring patient outcomes: capability (the ability for patients to do what is important to them), comfort (relief from emotional and physical suffering), and calm (reducing the chaos of navigating the healthcare ecosystem).2
In the U.S., improving patient-centered outcomes has become a highly discussed topic with ABIM’s Choosing Wisely program3, American College of Physicians’ High Value Care initiative4, and even major publications like the American Journal of Medicine’s recurring column on high-value care practice.5 In response to escalating healthcare costs, the Centers for Medicare & Medicaid Services (CMS) and other payers have shifted from traditional fee-for-service payments to value-based reimbursements such as the CMS Merit-Based Incentive Payment System (MIPS).6 Value-based health care empowers the clinician-patient relationship, places care delivery decisions at the expertise of a coordinated clinical team, and focuses on outcomes that matter most to patients.
The leadership of professional organizations, such as the Texas Medical Association (TMA), is invaluable to the process of defining and upholding the principles of value-based health care for systems and individual practitioners. Current TMA policy recognizes the need to advocate for high-value care principles in undergraduate and graduate medical education (Res. 201-A-18)7 and the adoption of the Choosing Wisely campaign (265.023).8 Although the evidence-based model (265.018.)9 previously adopted by the TMA does not encompass the full principles of the value-based decision making model, TMA resolutions on Cost Effectiveness (110.002)10 and Cost Containment (110.007)11 reinforce the need for cost-effective utilization of care.
On the federal level, exceptions to key legislation have been enforced recently to further advocate for value-based healthcare options. In November 2020, the CMS and Department of Health and Human Services Office of the Inspector General (OIG) released new exceptions to the Anti-Kickback Statute and the Stark law, effective January 19, 2021. These exceptions now allow more providers to participate in coordinated and value-based care arrangements that can improve quality and outcomes, lower costs, and increase health system efficiency, without the fear of severe criminal or civil legal backlash.12
The practice of value-based health care, although strong in theory, is not without flaws. The primary weakness of this system is that physicians are often responsible for things out of their control, such as referred providers’ costs and pre-existing conditions.13 This system requires widespread buy-in from all providers in order to collectively reduce costs and increase quality of care—effectively changing the culture of health care. Notably, this system inherently disincentivizes caring for patients of low socioeconomic status, particularly minorities, who inevitably generate higher costs due to health disparities.14 Weinick et al. emphasize adding a metric to the value-based healthcare system that addresses equity in health care. Their guide illustrates how to utilize value-based health care to reduce racial disparities, primarily by appending equity in pay-for-performance models.15
Goals of the Medical Student Section include staying informed about current policies regarding value-based health care since these policies are constantly changing and significantly affect reimbursement rates. Medical students are afforded the opportunity to learn about the principles of value-based health care from the very beginning of their training. Knowing the alphabet soup of value-based care (MIPS, APM, MACRA, etc.) will benefit patients and providers alike by improving outcomes, reducing costs, and maximizing reimbursements. In an effort to emphasize value-based health care early in the practice of medicine, the American Board of Internal Medicine sanctioned the Dell Medical School Value Institute for Health & Care’s STARS (Students and Trainees Advocating for Resource Stewardship) program. Over the past few years, student representatives across the country have met to learn about the principles of high-value care, review the Choosing Wisely campaign, and start their own initiatives at their respective medical schools. In Texas, students at UTHSC San Antonio’s Long School of Medicine created an ongoing Value-Based Health Care elective and degree distinction pathway. Dell Medical School offers online instructional modules and is a leader in patient-centered outcomes research. Medical students have a tremendous opportunity to impact high-value care through education, research, and student-led initiatives.
References:
Porter ME, Teisberg EO. Redefining Health Care: Creating Value-Based Competition on Results. 2006. Boston, MA: Harvard Business School Press.
Liu TC, Bozic KJ, Teisberg EO. “Value-based healthcare: person-centered measurement: focusing on the three C’s.” Clin Orthop Relat Res. 2017;475:315–317.
“Value-Based Health Care Must Value Black Lives,” Health Affairs Blog, September 3, 2020. DOI: 10.1377/hblog20200831.419320
Weinick, Robin & Rafton, Sarah & Msw, & Walton, Jim & Do, & Hasnain-Wynia, Moderator & Flaherty, Katherine & Scd,. (2021). Creating Equity Reports: A Guide for Hospitals.
In 2019, 18% of Texans had no form of health insurance.1 650,000 Texans have lost their health insurance due to unemployment during the pandemic. The rate of uninsured Texans is staggering and has only been worsened by the pandemic. During this critical time, we must talk about Medicaid Expansion and the potential solutions for millions of people with no health insurance. As a medical student, I have seen patients defer life-saving medications such as insulin in order to afford rent or groceries. Consequently, these choices have brought such people to the Emergency Room in diabetic ketoacidosis, which could have been easily avoided with regular insulin treatments. Stories like this are far too common in Texas, and it is important to recognize such outcomes are easily preventable with improved access to health insurance coverage. How can we as students learn to treat people, when the system we are bound to practice in is perpetuating their very diseases?
Retrieved from Texas Comptroller
Medicaid is a health insurance program managed through the Federal Centers for Medicare and Medicaid Services (CMS). Medicaid is currently jointly funded by the Federal and State governments with the Federal government matching each dollar the State spends. Texas Medicaid is primarily a fee-for-service model that has poor reimbursement rates and high administrative burden that discourages physicians from accepting Medicaid in their practice. Currently, Texas Medicaid coverage is only offered to children, pregnant women, seniors, and people with severe disabilities, who also fall below a certain income threshold. For example, a single mother making minimum wage at her full-time job is not eligible for Medicaid because she earns too much. However, she does not qualify for Federal subsidies covering some of the insurance cost because she does not earn enough. The Patient Protection and Affordable Care Act of 2010 would help address this woman’s dilemma since Medicaid Expansion would cover all individuals with incomes up to 138 percent of the Federal Poverty Level, amounting to $16,643 for individuals and $33,948 for a family of four. Medicaid Expansion would provide a health insurance option to an estimated 2.2 million uninsured low-wage Texas adults.2
Although the original arguments against Medicaid Expansion in Texas focused on States’ rights and limiting Federal dependence on funding, the primary opposition to this program was the Federal mandate. In 2012, the US Supreme Court ruled that the Federal government could not mandate the Expansion of Medicaid in any State, leading to Texas and several States opting out of the program. Realizing the benefits and improvement in health outcomes, several States have since adopted the Expansion program offered through CMS, including Arkansas (2014) and Louisiana (2016). Currently, Texas spends nearly $40 billion (State and Federal funds) for the Medicaid program, with a 60-40% distribution between the Federal and State Government respectively.3 Expansion would be fiscally sound for Texas as it will reduce the strain on our State budget and draw in more Federal resources. Looking past the dollar amount, it is crucial that medical students and other healthcare professionals recognize the benefits of improved access and early medical intervention that can be achieved through Medicaid Expansion.3
TMA’s Legislative Recommendations4
Develop a meaningful, statewide health care coverage initiative using federal dollars to:
Extend meaningful coverage to low-income uninsured working-age adults, and
Establish a state-administered reinsurance program to reduce premiums for people enrolled in marketplace
Provide 12-months’ comprehensive coverage for women who lose Medicaid 60 days
Establish 12-months’ continuous coverage for children enrolled in Medicaid, the same benefit given to children enrolled in the Children’s Health Insurance Program.
Accounts TCof P. Uninsured Texans. Retrieved from- https://comptroller.texas.gov/economy/fiscal-notes/2020/oct/uninsured.php
Beyond borders, beyond languages, and beyond our differences students across the world have united with a common purpose to serve and create a positive impact. With over 1000 students comprising more than 90+ countries, #Students_Against_COVID, a grassroots movement has served as the cornerstone for creation, purpose, fulfillment and fostered collaborations throughout the world allowing students to join forces in the fight against the COVID-19 pandemic.
#Students_Against_COVID Volunteers, Friends & Family
The Power of Technology
The Spanish Flu or the 1918 pandemic over 100 years ago, vastly differs from the COVID-19 pandemic due to the availability of technology. Since then, there have been many advancements with new medical equipment and instruments to care for patients. Many cures for diseases or drugs that were impossible decades ago are now a reality due to the hard work and diligence of researchers in finding answers to the centuries’ old medical mysteries. During the Spanish flu pandemic, scientists could hardly imagine elucidating the nucleotide makeup of the virus, but with the advent of polymerase chain reaction (PCR) half a century later, in today’s technological landscape, within 2 weeks of a global emergency scientists were able to determine the sequence of the coronavirus genome. Within seconds, a text message from South Africa is transferred via the internet to Canada, and as such the spread of information and misinformation has appeared to be an added pandemic, namely the infodemic of the century.
Objectives of SAC, the Grassroots Movement
One of the core objectives of SAC in tackling the infodemic and the pandemic, has been to disseminate trustworthy information as quickly as possible and in as many languages to reach minorities, villages and people far away. From Pashto in Afghanistan, Turkish in Turkey, German in Austria, Hausa in West Africa, Yoruba in Nigeria to Lugada, the most prestigious language in Uganda, “the Pearl of Africa”, students have translated different COVID-19 campaigns.
Social Media Campaigns Translated
The objective of the Global Health & Social Media Team has been to echo public health guidelines to stop the transmission of the infectious disease and to encourage those with symptoms of COVID-19 to seek medical assistance. Despite the socio-economic challenges for many without access to the internet, the major global health challenges the international community face will require an integrated, interdisciplinary approach addressing the political, cultural, legal, biological, and medical issues. Therefore acknowledging the role of technology in tackling the ongoing pandemic the team aims to eliminate avoidable disease, disability and death, while serving as an avenue of health promotion and disease prevention.
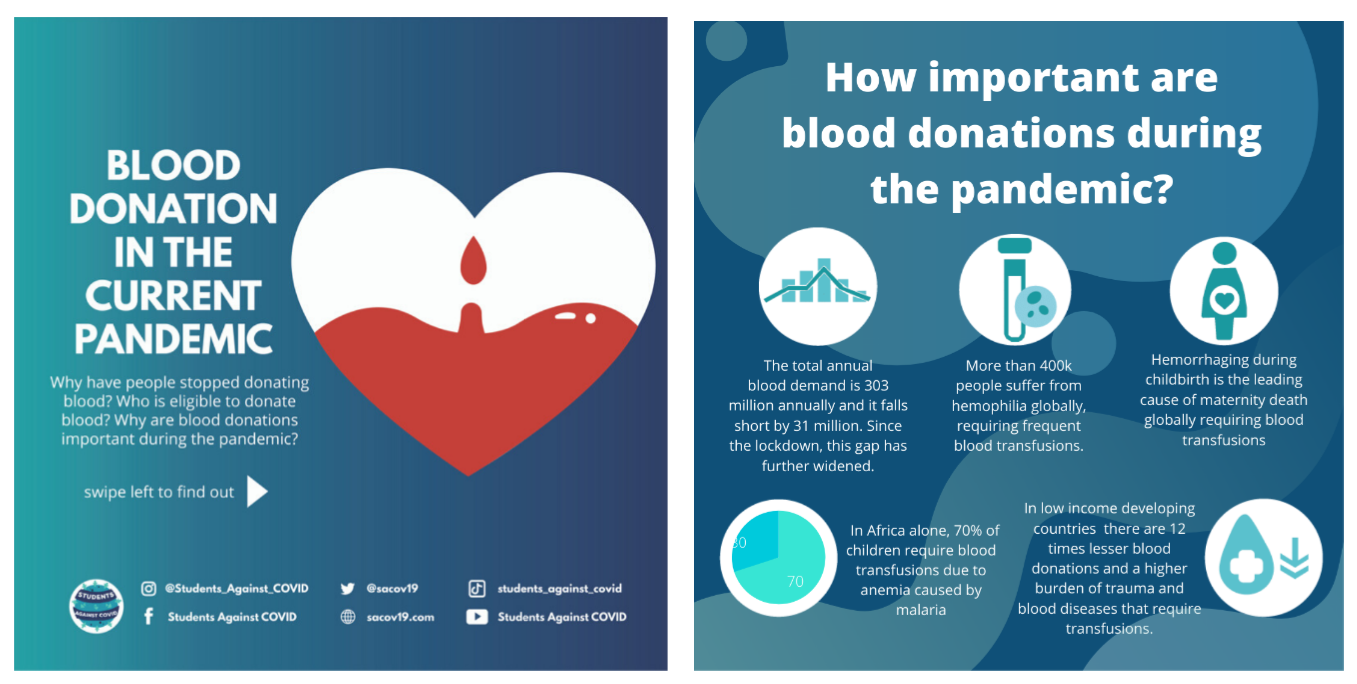
Blood Donations Campaign
As such, important values, such as altruism, service in times of crisis, and solidarity with people around the world offered the chance, or opportunity of a lifetime to participate in the fight of this historic pandemic. Stemming from leadership’s most fundamental element to create a difference in the lives of others SAC therefore provided students with a platform to unleash their creativity and innovation necessary to navigate a crisis and to emerge from it healthy.” by Leah Sarah Peer
Additionally, with increased reliance on virtual platforms for connection and socializing, telehealth technologies for consultations, counseling sessions and physical examinations, physicians have been able to continue providing care while maintaining social distance. Similarly, educational institutions have transitioned to online remote learning where students and professors meet over interactive technologies such as Zoom and Google Meets for lectures. Medical students especially have had their clerk-ships suspended without direct patient contact while others have graduated early to serve as front-line clinicians. In this manner, technology has defied space and time, as it has not only exposed the fragility of humanity but also proved that technology is an integral part of our future evolution.
Women’s Health Team
A Spark of Creativity & Innovation
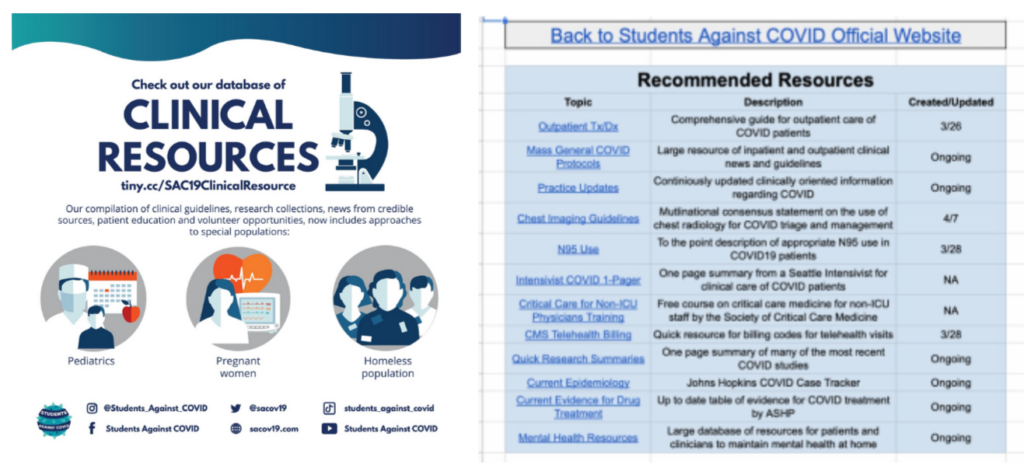
With more free time for students, as the usual commutes to school, scheduling of classes and extracurricular in person activities were all cancelled they were able to invest in themselves and even develop new hobbies. Within SAC, it was evident that despite the negative impacts on medical education, these exceptional times represented opportunities for change. Such an example is that of the Clinical Resources Team, that curated a database of clinical resources for health professionals to access COVID-19 & medical information. This volunteer experience among many highlighted the value of non-graded elective courses in furthering student’s knowledge while allowing them to participate in a movement greater than themselves. As such, important values, such as altruism, service in times of crisis, and solidarity with people around the world offered the chance, or opportunity of a lifetime to participate in the fight of this historic pandemic. Stemming from leadership’s most fundamental element to create a difference in the lives of others SAC therefore provided students with a platform to unleash their creativity and innovation necessary to navigate a crisis and to emerge from it healthy.
Besides making a difference, SAC provided a sense of community where friends soon became family. In isolation many were reminded of our collective values and collective history, emphasizing society at large rather than individual self-interest.
The Mental Health Team sparked the beginning of students inspiring one another, of sharing their own stories as well as becoming listeners as a crisis naturally triggers a range of physiological and psychological responses that are heightened under lock-down. The earlier trauma and abuse students faced often resurfaced as the lost sense of normalcy triggered grief with feelings of denial, anger and depression.
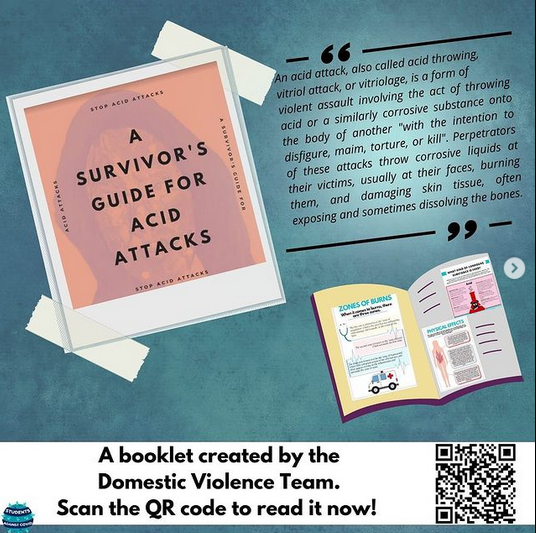
Women’s Health Team Activities
Bearing the consequences in mind, the Women’s Health Team of SAC drafted up a list of domestic violence hotlines per country for individuals afflicted by domestic violence. To them, having access to these resources during quarantine was vital and therefore have further created campaigns on sexual health, reproductive rights, maternal health and “The Period Project”, all aiming to raise awareness for the challenges girls and young women are faced with. Passionate about women’s health, to commemorate international breastfeeding week, educational material was prepared celebrating womanhood while promoting access to skilled breastfeeding counseling.
Advocating for Vulnerable Populations
Nonetheless, the #Students_Against_COVID community rarely sleeps and while students are taking care of themselves, and those around them, they are also actively advocating for vulnerable populations.
The Asylum Seeker’s & Refugees initiative within SAC aims to raise awareness about the predicament of minorities by creating infographics, and posters. Furthermore, underway is the curation of a database of World Organizations & Charities for donations so that donors have access to places where their funds are needed and may be used wisely. In a catastrophe such as that presently in Lebanon, the database gathers recognized Lebanese Non-Governmental Organizations (NGOs) providing humanitarian aid and emergency relief.
Co-Leads of the Asylum Seekers & Refugees Initiative Shedding Light on the Yemen Humanitarian Crisis
Additionally, bearing in mind the challenges of the COVID-19 pandemic, the team recognizes the plight of refugees suffering from human rights violations. Whether forced to leave their homes, their communities and their families, to find safety in another country, the Asylum Seekers & Refugees Team within SAC abides by the Universal Declaration of Human Rights (UDHR) to assure all human beings are treated with respect and dignity. Since, by definition, refugees are not protected by their governments, the international community steps in to ensure the individual’s rights and physical safety while monitoring and promoting respect for refugee rights. Although the newest edition to #Students_Against_COVID family, the team’s aim is to strengthen and broaden public information, education and involve members of the civil society in refugee, asylum seekers and migrants protection.
Recognized for it’s positive contributions internationally, #Students_Against_COVID was awarded the Pollination Project grant, won 1st place in the DICE Foundation COVID-19 Innovation Challenge, as well as the 2021 CUGH Pulitzer Prize for Highest Impact Project, Video Submission.
#Students_Against_COVID Global Health Program
Besides these accomplishments, currently in the works and set to launch late spring to early summer 2021, is the creation of a unique, Global Health Program: An interdisciplinary Overview. It’s aim is to cultivate a better understanding of Global Health amidst the COVID-19 pandemic and the program hopes to connect global health enthusiasts from around the globe, introducing students and young professionals to critical global health issues and ways to address or solve them.
Happy New Year 2021 – A Recap & Reflection of the Movement
As the crisis evolves, compassionate leadership entails the unified efforts of changemakers championing science in both local and international theaters. Although words may not adequately serve to express the work and dedication of this virtual agora, pushing boundaries to inspire, help and motivate people is at the centre of the #Students_Against_COVID movement!
Leah Sarah Peer is a medical student at Saint James School of Medicine in Chicago and a graduate of Concordia University, Specialization in Biology, Minor in Human Rights in Montreal, Quebec, Canada.As a Core-Facilitator within Students_Against_COVID, Leah aims to foster belonging and inclusion to unify the movement and compassionately strives to empower others to make a difference.
Societies across the world have been disrupted by the Covid-19 pandemic, with millions of people being forced to stay indoors and many losing their jobs. But this very disruption has ushered us into what could be the new future of work. Remote work itself has been around for years but, traditionally, companies prefer their employees to work at their physical headquarters. That’s all beginning to change as a result of the pandemic.
With no choice for companies, entire industries and employees alike were forced to embrace remote work—yet this may just be the beginning. In fact, Business Insider recently discussed 12 different companies that were extending remote work, with some end dates as far away as the summer of 2021.
For other industries, however, there may not even be a return to the office on the horizon.
Technology has made remote work possible but, ironically, has also been a disruptive force that has uprooted traditional jobs. This trend has only been accelerated by remote work—employers have realized just how many jobs can be done from the comfort of their homes.
Over the past few years, the medical field has been slowly merging with technology. Every aspect of the healthcare system, from entire hospitals to physicians, is being influenced by new technological trends, including remote work. The future of the field has never been more unclear.
Flexibility with Administrative Tasks and Employees
In the coronavirus era, medical professionals are in high demand for obvious reasons. Many medical facilities have transitioned to working remotely. In fact, the automation of administrative tasks has been a major byproduct of the Covid-19 pandemic.
Offices around the country report feeling positive overall about these changes. Medical Economics recently examined Lugo Surgical Group, based out of Texas, who have been operating remotely for two years, showing that this is viable.
Each week, the owner of this clinic, Rafael Lugo, reserves a day and a half to meet with patients. Every other aspect of the surgical process—including billing, scheduling, and follow-ups—are done remotely.
While doctors and nurses still need to meet with patients in person, it is clear that this is not the case for administration. This new hybrid business model has altered the jobs available in the medical field. In fact, the Bureau of Labor Statistics projects a 9% decline in secretarial or administrative assistant jobs over the next decade. Nonetheless, Covid-19 has highlighted the need for in-person physicians but has demonstrated that administrative workers are not essential for the office.
The Emergence of Artificial Intelligence Systems
While admin roles may be on an accelerated decline due to Covid-19, their replacement is coming far quicker. Artificial intelligence systems are impacting every field of business and its impact on medical practices is profound. Handling administrative tasks is just the tip of the iceberg for these advanced systems; however, there is a downfall. The trust medical offices have placed on these systems during the pandemic may result in them relying on AI to handle more intricate jobs.
As such, AI is changing medical practices, particularly when it comes to patient care. Surgeries powered by robotic instruments that are controlled by a surgeon are becoming extremely popular, and some systems are now able to diagnose patients quickly based on information inputted in the system. As these systems continue to develop, new jobs will open in the field of medicine based on regulating this technology and developing it.
Entire companies may form, focused on developing and then producing these AI and robotic systems. DaVinci Systems is a modern example, as the company produces surgical robots that are controlled via a human surgeon at a desk. These devices have already been approved for urological procedures, radical tonsillectomy, and even tongue base resections. Remote work has shown a new way in which these systems can be helpful. In truth, this pandemic could very well result in a future where there isn’t even a human surgeon behind the robot.
Altering Career Paths and Customer Expectations
Before the pandemic, a common headache for patients was the annoying wait times and variability in the quality of service provided by the doctor. During the pandemic, though, wait times have become non-existent, with medical professionals able to conduct their job over a Zoom call. Additionally, the advancements of artificial intelligence systems could result in more accurate diagnosing in the future. Having access to medical professionals wherever and whenever, however, may have its drawbacks—patients may become disgruntled if medical practices return to normal after the pandemic settles.
As for doctors and other medical practitioners themselves, Covid-19 isn’t just changing the way they work, but also how they progress in their career. Online nursing programs, offered by accredited schools such as Johns Hopkins University and Rutgers University, have become more popular during this pandemic. With the number of people earning their degrees online increasing, remote learning practices may ease the transition to remote work. This could also contribute to the industry-wide switch over to automation powered by artificial intelligence.
Covid-19 has changed the way entire industries operate and the medical field is no exception. From artificial intelligence replacing administrative jobs to the way budding practitioners are learning the ropes, reliance on technology has increased as a byproduct of the pandemic. This is likely to lead to a future where medical practices are largely automated and in-person visits to the doctor are disrupted by robotics.
Based on current trends, these changes were inevitable, but the pandemic may have accelerated them. While the future of the coronavirus is unclear, its effects on the workforce and jobs may be permanent—the way work is handled could be disrupted forever.
Doctors are men who prescribe medicines of which they know little, to cure diseases of which they know less, in human beings of whom they know nothing.” – Voltaire
The covid-19 pandemic has claimed millions of lives, shut down economies, restricted movement and stretched our healthcare systems to the edge; but despite this time of destruction, Peer Med, a podcast dedicated to serving humanity was born! Established as a platform for creation, innovation and above all a platform for unity.
A student-led initiative of the Peer Medical Foundation, the Peer Med podcast intertwines medicine, an ever changing science of diagnosis and treatment, with conversations about issues in healthcare where lives are on the line. Due to the fashionable focus of medical education on biology, pathology and disease there has been a reduced emphasis on the social determinants of health. As such physicians lack an empathetic character understanding the human aspect of medicine and in this, fail to communicate effectively rendering patients dissatisfied with care.
Seeing the need for more fruitful discussions, the Peer Med Podcast provides listeners with a more nuanced interpretation encouraging health professionals to look beyond medicine and into the experiences, values and beliefs of patients to assure a successful therapeutic relationship. It serves as a reminder of the importance of self-determination, beneficence, non-maleficence and justice as medicine naturally exposes health professionals to the darker side of human existence. The podcast explores these themes by delving into the underbelly of life where homelessness, drug addiction, abuse, trauma, and death are brought to the surface of conversations. It takes the already prevalent cases of strokes, pneumonia, heart attacks, fractures, and miscarriages from the everyday scenarios in emergency rooms plaguing our species and encourages a more humane outlook amidst all conflict and chaos.
“Doctors are men who prescribe medicines of which they know little, to cure diseases of which they know less, in human beings of whom they know nothing.”
– Voltaire
Founded on March 24th at the start of the COVID-19 pandemic, Peer Med is dedicated to humanity and the millions of people worldwide without access to education, health and water, sanitation and hygiene (WASH) services. The podcast aims to inspire, engage and promote action to solve challenges in global health, human rights and medicine. Acknowledging that the delivery of healthcare requires a team effort, the podcast invites everyone from clinicians, advocates, economists and even comedians to delve into the subjects of medicine. While peer-reviewed information is important, not all valuable work belongs in an academic journal. In order to strengthen health systems a multidisciplinary set of perspectives is required to teach and inspire people. Therefore, Peer Med encourages dialogue so that all listeners may raise their voices advocating for humanity.
Ensuring Peer Med is truly a global podcast is the goal but despite the best intentions to ensure inclusivity, barriers in terms of gender, language, and access prevent this from happening. To tackle the problem, Peer Med aspires to invite speakers from all corners of the world, not only to assure equitable representation but to also gain advice on how to empower those in low-and-middle-income-countries (LMIC) so that their voices may be heard. In serving humanity, Peer Med is completely free and available on a variety of platforms aiming to leave listeners refreshed, empowered and motivated to effect change. These can be heard from a mobile phone, shared via social media, or played for a friend. The conversations will leave listeners burning with a flame in their hearts to do their utmost on life’s quest to serve humanity.
It serves as a reminder of the importance of self-determination, beneficence, non-maleficence and justice as medicine naturally exposes health professionals to the darker side of human existence. The podcast explores these themes by delving into the underbelly of life where homelessness, drug addiction, abuse, trauma, and death are brought to the surface of conversations. It takes the already prevalent cases of strokes, pneumonia, heart attacks, fractures, and miscarriages from the everyday scenarios in emergency rooms plaguing our species and encourages a more humane outlook amidst all conflict and chaos.
Leah Sarah Peer
The support for the podcast has been humbling as love has poured in from around the globe. So many are keen on sharing their stories and this speaks volumes to the passion of the podcasts’ guests, their enthusiasm and commitment to mankind. Some have included a world renowned speaker and human rights champion, a Brooklyn-based singer, songwriter, teacher and PhD candidate in Comparative Literature, a range of student initiatives – Meet the Need Montreal, Helping Hands, to Non-profit Organizations such as Med Supply Drive and so many more.
If there is something the COVID-19 pandemic has taught us, it’s the power of community and compassionate care’s strength in uniting us across the world. Peer Med hopes to serve as a medium for inspiration, for reflection, and invites people from across the healthcare spectrum to come together committed and dedicated to serve humanity.
To listen to Peer Med, visit Spotify, Apple Podcasts. To read about the individual episodes visit the website for more.
Before I embarked on my second year of medical school, I wanted to try something different — an experience I probably wouldn’t attain during the medical school curriculum.
I have always had an inquisitive mind, hence research held a natural appeal. Research, at least to me, can be broadly categorized into two groups: dry lab and wet lab. I was already involved in the former, but was keen to give the latter a shot. An oncologist took me under his wing, and I was soon introduced to the world of lab-based, experimental research.
Coming from a background with literally no lab experience, it was undoubtedly a steep learning curve at inception. There was an avalanche of lab-based skills I needed to learn and understand. I was tasked to perform lymphoma research, but it wasn’t until a month later that I actually got to perform experimental work on lymphoma cells. The first month was humdrum but necessary. I had to complete multiple safety courses, practice micro-pipetting, and learn about the entire range of complex lab equipment and procedures such as the centrifuge, film development for western blots, and flow cytometry machine.
After one month, I was given my topic and tasked to draft the experimental protocol. In brief, I was investigating complement-mediated cytotoxicity of rituximab (anti CD20 monoclonal antibody) on lymphoma cell lines. Even though I had some prior knowledge about the cytotoxic mechanism, I had to perform an in-depth literature search to augment my understanding and look for existing experimental protocols that I could potentially adapt.
With a protocol in my armament, I thought I was confident and equipped enough to perform the experiment, until I realized that multiple roadblocks lay ahead of me. An initial protocol with six simple steps turned out to be twice as long after adding several intermediate steps that I had missed. There were other reagents that I had to add. For instance, staining the cells involved identifying the appropriate stain color, optimizing the concentration of the stain solution, incubating it for a period of time; it was not as simple as adding a reagent to a test tube of cells. Hence, it often took longer than expected to complete a single step, which resulted in me being late for the equipment bookings. Time management was the first lesson for me. It was quintessential for me to plan, in detail, the total amount of time I actually needed per step, with some degree of overestimation.
The road ahead was filled with pockets of ups and downs, albeit often the latter. There were many occasions on which experimental results contradicted my hypothesis – cells died when they were not supposed to; cells didn’t die when they were supposed to. When occasions like these arose, I went back to scrutinize every step in the protocol, to make sense of what could have possibly went wrong. But I soon realized that the things that seemed insignificant to me were the sources of the experimental failures. For instance, I had initially assumed that all serum types were similar in composition and purpose. However, the serum I had used was not viable for cell survival. Hence, I switched from commercial serum to human serum in subsequent experiments. The next road block came when my cells became unresponsive to rituximab. It was only much later on that I accidentally happened upon a paper, which stated that the particular cell line in my experiment was intrinsically resistant to the drug. These experimental failures served to teach me one very important lesson — to scrutinize the fine details and consider every possibility that could account for failures.
Lastly, I would like to underscore the significance of perseverance. I consider it to be the cornerstone of being a good scientist and researcher. Amidst the myriad of failures, I would have given up on continuing my experiments if I was devoid of it. Research can be a plodding process with multiple failures; but if you believe in your purpose and persevere, you will eventually reap the fruits of your labor.
I have always had an ardor for research, and I intend to pursue the Clinician-Scientist pathway. I am thankful for this lab experience, for it has opened my eyes to the unappealing — at least to most medical students —world of research. As mundane as it can be, I find both the process and end product meaningful to fellow scientists, doctors, and the society at large. This experience has not stifled my interest and passion for research and science; it has taught me instead the values that are essential for a scientist.
If you’re thinking of doing research or being a clinician-scientist, this is just my two-cents worth of lessons that I’ve personally picked up in my short five month stint thus far in the lab. Be humble. Be hungry to learn. Be careful to look out for details. And, most importantly, persevere despite how monotonous research can be.
Almost everyone has seen a doctor at some point in their lives. Yet, for most, what actually goes on in medical school remains a mystery. Chances are that if you’re reading this, you have experienced the delightful experience that is medical school. Sleeping in late, eating well, and relaxing with friends and family on the weekend are just a few of the joys that we medical students get to experience. Just kidding. Medical school, as most of us know, is beyond challenging. At my school, faculty members fondly liken the medical school experience to drinking from a fire hydrant. As medical students, our pre-clinical days are comprised of hours and hours of lectures and power points. Then, when class is all over, we get to top off the day with several additional hours of studying. It’s challenging, it’s overwhelming, and at times, it seems downright impossible.
Part of what makes medical school such a unique challenge is the fact that medicine is a tactile discipline and yet, pre-clinical education is traditionally taught in a classroom setting. In response to this dichotomy, the University of Vermont’s Larner College of Medicine recently made headlines by announcing that it would become the first public American medical school to completely eliminate lectures from its curriculum, joining private Case Western Reserve University School of Medicine in Ohio (https://www.washingtonpost.com/news/to-your-health/wp/2017/07/29/medical-school-without-the-sage-on-a-stage/?utm_term=.6847516c2b31.) This change, which is expected to be fully implemented by the year 2019, comes in response to concern that the traditional lecture format does not promote knowledge retention and instead relies on “passive” learning where the learner is not actively engaged in their education. To draw an analogy, passive learning is like being fed while active learning requires learners to pick up the fork to feed themselves.
Although the University of Vermont and Case Western Reserve University seem to be the only two institutions whose medical schools have committed to becoming completely lecture-free, it’s interesting to realize that other schools have moved towards a more active learning format as well. In my school, the College of Osteopathic Medicine of the Pacific (COMP) , students pick their own small groups. These small student-led groups meet several times a month and work together to complete assignments and discuss scenarios that are based upon real clinical scenarios. Northwestern University’s Feinberg School of Medicine is one of several schools that employs a problem based learning curriculum, and in 2015, Harvard Medical School also restructured their curriculum to become more problem-based. Ultimately, medical school curriculums exist on a spectrum from passive to active curriculum styles and the continuum seems to be shifting to favor active learning styles at many medical institutions.
Moving away from a traditional lecture setting certainly presents its own unique challenges that affect learning. The non-lecture curriculum requires more self-reliance on the part of the students, who must teach themselves new material. The small groups used at COMP, for example, are completely student-led. A faculty member may pop in for a few minutes to make sure that the group is running smoothly, but often these faculty members are not experts in the subject matter at hand and are present to deal more with administrative issues than to teach content. It also means that students are required to participate in groups, whereas many schools may have optional attendance for lectures. Perhaps the biggest challenge of the active learning curriculum, however, is the necessity for different personalities to work together to achieve a common goal. The traditional classroom setting involves one teacher who employs a specific style to reach multiple students. In the active learning curriculum, small groups are often used, in which each member has a different personality. Students in these groups must work together, sometimes despite personality differences, to master the curriculum and achieve common goals. Although the group setting closely resembles the team-based approach taken in most healthcare settings, it can undoubtedly be frustrating, especially for someone like myself who tends to be more introverted and likes to study on his/her own. In my personal experience, the members of my small group were incredibly supportive and had a variety of strengths, yet there were many days when I couldn’t wait to return to the comfort of my own room to be able to really learn the material myself. Sometimes trying to learn unfamiliar concepts with others was a distraction, and despite the best of intentions, small group was like the blind leading the blind when we were all confused on certain concepts. There were some times that the small group felt comforting, like someone holding my hand, and other times when it felt too overwhelming, like someone pressing my face up against that proverbial fire hydrant. Ultimately, I felt like the combination of both lectures and small groups was actually more dynamic than relying solely on one or the other. While the University of Vermont and Case Western Reserve University have both made the bold move to abstain from lectures altogether, they join the company of many medical schools, both allopathic and osteopathic, that have recognized the importance of active learning for the medical school curriculum. Let me know what alternatives your medical school offers to traditional lecture-style learning!
In a world where drug companies and pharmacies remain pervasive, an innovative take on the word “pharmacy” is being developed in Redwood City, CA. A new food pharmacy has just opened up, stocked with fresh fruits and vegetables. Just what the doctor ordered – literally! Instead of paying supermarket prices for these foods, all you need is a prescription from the doctor.
The first of its kind, this food pharmacy is an annex to the existing Redwood City free clinic known as Samaritan House. Patients with type II diabetes can get a prescription for fruits, vegetables, and even fish from a physician, and then pick up the free food at the pantry to help better manage their diabetes. The food is procured and delivered by the Second Harvest Food Bank, which is one of the largest food banks in the nation, feeding almost a quarter of a million people each month. Second Harvest also provides nutritious cooking demos given by local nutritionists1.
This one-year pilot program serves as a reminder that food is often overlooked as a primary method of treatment and prevention; a reminder we might need during our incessant drive to memorize pharmaceuticals and their mechanisms of action. Even when it is known that a patient’s congestive heart failure and diabetes may not be adequately controlled long term by medication alone, oftentimes physicians are strapped when it comes to options. Providing education on proper nutrition to a patient who simply cannot afford fruits and vegetables remains the passive and limited option, whereas food pharmacies such as Samaritan House are active steps in the right direction.
Human head transplantation (the head anastomosis venture project – HEAVEN) has been for a long time merely a neurosurgical and medical theoretical concept that did not enjoy much attention among the medical community. However, in recent times, there have been voices trying to revitalize this question. Italian neurosurgeon, Dr. Sergio Canavero, is one of the most prominent protagonists in this regard. The idea behind this concept is to help people who have severe physical disabilities (such as neuromuscular dystrophies or tetraplegia), but have an intact head and brain. There is a vast array of medical, ethical and physiological questions and obstacles that are ahead of this endeavor. Despite a lot of skepticism, Dr. Canavero has laid out a couple of transplantation protocols he believes can get the job done. In these protocols, he tried to answer and address every possible challenge that is expected to occur during this delicate and immensely complex procedure. The main purpose of this short article is to analyze the crucial components of his protocols and try to determine if they have any rational scientific relevance and ethical/medical justification.
Why do it?
Before you chop someone’s head off, you’d better have some good reasons, right? This is fundamental. In medicine, conditions are treated if the potential benefits of the treatment outweigh the potential risks. For each particular disease state, there has to be a justified medical indication and logical/rational foundation behind treatment. This is the sine qua non of every medical intervention. You have to bear in mind that anything you do has to lead, ultimatively, to a better quality of life. In that regard, I doubt that this procedure would accomplish that goal at the present moment and it principally acts as an academic exercise, albeit lethal one. I generally do not support doing things just for the sake of doing them, especially in medicine where such behavior can be costly and unethical. Sure, you can become hero of the day and act in a „told you so“ manner if things go your way, but what if they don’t?
Even if you theoretically manage to overcome the technical and technological barriers that are inherent to this procedure, the question still remains: will this person experience improved quality of life? Dr. Canavero’s logic is that people who suffer from severe and/or progressive neurological conditions, e.g. muscular dystrophy or quadriplegia, could potentially benefit from this procedure. How? Well, if your peripheral nervous system does not work but you do have preserved cognitive functions (brain and brain stem), then you would be able to theoretically join healthy brain with healthy body of a deceased donor. The idea is that this body would be donated by those people who were clinically confirmed as brain-dead due to, for example, severe head trauma, but still had a fully functional body to offer. On the other hand, the „recipient“ of the body would give an informed consent that he/she is willing to undergo a body transplantation procedure, regardless of a high risk that this procedure could end in death. In popular jargon – „people who have nothing to lose“ are the group of people that are targeted as candidates for this procedure in Dr. Canavero’s opinion.
Feasability
Dr. Canavero laid out 2 operative protocols that provide a theoretical framework for this type of experiment. One of them is called HEAVEN1 and addresses head-to-body anastomosis, while the other is named GEMINI2 and features a spine fusion protocol. The physiological obstacles that Dr. Canavero needs to overcome in order to succeed in this endeavour are tremendous, but I will try to briefly tackle the 4 major ones.
Brain perfusion problems – in only a few minutes post-decapitation, it is expected that neurons will be exposed to a hypoperfusive state, ultimately resulting in brain tissue death.
Fusion of two ends of the spinal tract – this has never been done before in humans.
Reparation and regeneration of neuronal connections and spinal tracts/projections within the CNS and the restoration of the motor and sensory functionality.
Post-transplantation complications – this includes potential tissue transplant rejection reactions that are immunologically mediated.
Should we do it?
At this point, we just do not know enough about the proposed procedures. Some of them have been performed on animal models and some were done only in a Petri dish. Results obtained through animal experiments and in-vitro molecular models might not correlate (and most commonly they don’t) with human physiology. In the early 1970s, American neurosurgeon Robert Joseph White performed the first monkey head transplantation onto a body of another monkey3. The recipient monkey lived for 8 days, and there were no surgical complications encountered. However, the monkey was quadriplegic since the surgical protocol did not address the problem of spinal fusion4. This resulted in a monkey who was completely paralyzed from the neck down, but who could still eat and follow objects with its eyes since the cranial nerves, brain stem and other brain structures were intact and perfused by the circulatory system of the donor’s body. Moreover, it was reported that the transplanted head could hear sounds and smell/taste food. However, immunologic reactions in the form of graft rejection ensued and the monkey died from them.
In this regard, Canavero’s protocol is essentially just a „compilation“ of biotech solutions for a wide spectrum of problems in medicine. Successful translation of any of these theoretical concepts into the clinical arena would be a giant leap in medicine. However, strictly lege artis, there is no strong evidence that these techniques will be successfull at all. Patients undergoing this procedure could be left in much more catastrophic and miserable conditions than those endured prior the procedure. Transplantation of a human head onto a new human body should not be perceived merely as transplanting a flower from one pot to another. We do not know how the brain would interact with the new neurochemical and biochemical milleu of the body that it just received. How would the brain integrate and process new signals arriving from the newly discovered periphery? How would the brain process perception and information coming from these new muscles and other body structures? These problems were emphasized in a recent letter written by Dr. Cartolovni and Dr. Spagnolo, published in the Surgical Neurology International journal. In this letter, the authors argue that Canavero’s perception of the human body functional framework is strictly mechanistic, and largely disregards the importance of body self-cognition, which plays a real part in the formation of human self.
Additionally, they state that head transplant procedures raise significant social and ethical problems in terms of organ donation. A leading medical ethicist, Dr. Arthur Caplan from NYU’s Langone Medical Center, states that the implications of this procedure are far-reaching and extremely dangerous from the ethical and medical standpoint. Similarly, Dr. Jerry Silver from Case Western University states that he perceives human transplants as a barbaric method at this point in time. Moreover, he said that he does not expect such procedures to be successfully performed for at least the next hundred years.
In my opinon, we are not ready for this type of procedure, at least in light of the most recent evidence-based medicine. Even if the tremendous technical difficulties could be surpassed, it still remains a question how the brain (center) would integrate with the periphery. At this point, I assume that the brain would be overwhelmed with the amount of input that it would receive from the periphery, ultimately leading the transplant recipient to derangement, pain and insanity. The prospects of this experiment are simply grim and unfavorable, with our present knowledge and, therefore, I would advocate for its halt.
References
Canavero S. HEAVEN: The head anastomosis venture Project outline for the first human head transplantation with spinal linkage (GEMINI). Surg Neurol Int. 2013;4(2):S335-42.
Canavero S. The „Gemini“ spinal cord fusion protocol: Reloaded. Surg Neurol Int. 2015;6:18.
White RJ, Wolin LR, Massopust LC Jr, Taslitz N, Verdura J. Primate cephalic transplantation: Neurogenic separation, vascular association. Transplant Proc. 1971;3:602-4.
White RJ. Hypothermia preservation and transplantation of brain. Resuscitation. 1975;4:197-210.
Čartolovni A, Spagnolo AG. Ethical considerations regarding head transplantation. Surg Neurol Int. 2015;6:103.