Why as a society is difference viewed as unattractive?
By Lauren Higgins




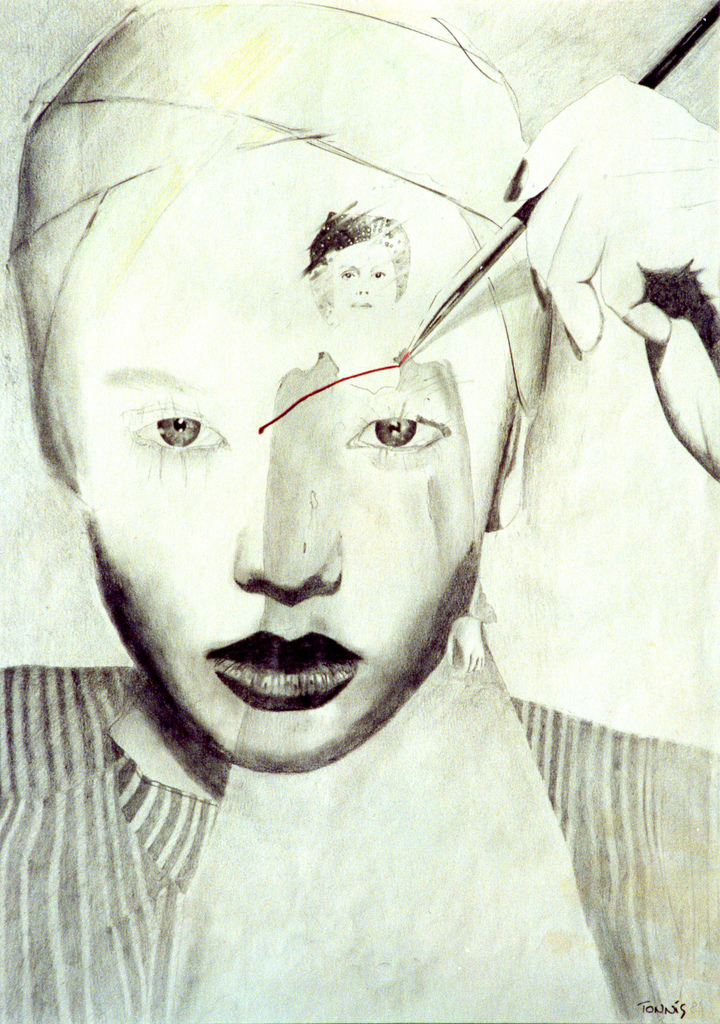
Cherri (2022) The Adoration of the Golden Calf
The artefact I have selected is a lamb taxidermy called, ‘The Adoration of the Golden Calf, after Poussin’, which was created in 2022 by Ali Cherri and finished using wood, jesmonite and gold leaf.
The piece was commissioned in 2021 as part of the National Gallery Artist in Residence programme and sat within the Sainsbury wing of the art museum as part of the ‘If you prick us, do we not bleed?’ project. This exhibition focused on historical pieces which had been vandalised when displayed, with Cherri assembling individual artworks to reflect the trauma of the original. This taxidermy of a lamb that died due to severe birth abnormalities, specifically relates to the Golden Calf depicted in the work of Poussin, which was destroyed with spray paint in 2011 (Wilson, 2011).
This unusual, alien-like figure immediately captured my interest, as it stood in high contrast to the beautifully depicted biblical scenes of the Renaissance paintings which surrounded it. Centred within the gallery, I also noticed that this artefact had caught the attention of large crowds, with many recoiling in disgust and horror at the physical appearance of the lamb. It has often been deemed human nature to be captivated and intrigued by the unknown or different, however the pure hatred that was directed towards this piece simply due to its distorted appearance shocked and outraged me. I, therefore, began to consider the animosity that individuals who suffer from noticeable deformities face, and the challenges of living in a society that doesn’t fully accept those who are atypical.
The distinct characteristics of the lamb also reminded me of the infamous Siamese conjoined twins. I thought about the struggles they must have encountered not only due to the disability itself, but also the unwanted views and opinions of society at the time. I wondered whether after 100 years since their death if they would receive a similar reaction of repulsion which I witnessed being directed towards the abnormalities of this figure (Bahjat, 2018). Moreover, this sculpture encouraged me to reflect upon my own disability; the impact it has had on my life and the additional challenges I shall encounter as a medical student.
Throughout history, individuals deemed to be ‘medical oddities’, have been subject to curiosity from the public audience and even used as forms of entertainment for the so-called freak shows (Grande, 2010). The exhibition of extraordinary bodies occurred across Europe and America during the Victorian period, whereby physical difference was seen as a profitable market (Durbach, 2012). Chang and Eng Bunker, credited as the original Siamese twins, were examples of individuals showcased around the world for paying audiences (Bahjat, 2018). The Bunker brothers were attached at the breastbone via a ‘small piece of cartilage’, but each had their own set of organs and body, allowing them to carry out the activities of a normal man (Bahjat, 2018).
At just the age of 17, the brothers’ peculiarities were identified as having ‘commercial potential’ by Robert Hunter, who proceeded to buy the boys from their mother in Thailand and exhibit them across the globe (Leonard, 2014). The idea that the Bunker brothers, and so many other individuals with physical deformities, were used as amusement for others is deeply saddening (Kattel, 2018). The humiliating and dehumanising nature of freak shows makes me consider the psychological implications patients with physical disabilities must endure due to the strain of unsolicited comments and community opinions.
Alongside the link to the Siamese twins, the structural deformity of the artefact reminded me of my own physical anomaly. I have an idiopathic form of scoliosis, which is the lateral deviation of the vertebral column without a known cause (Martin and Law, 2020, p.692). As a result, I have uneven hips and shoulders, poor posture, severe back pain/ discomfort, and lowered self-esteem due to an obvious hump-like structure caused by the posterior raising of my ribcage (kyphosis). Similarly, to the ‘freaks’ of the 19th century, I have personally been subject to wondering eyes, judgmental expressions, and hurtful remarks about my appearance when out in public (Grande, 2010). I, therefore, have experienced first-hand the damaging mental health consequences indirectly connected to my disability.
Although my scoliosis has posed many additional challenges in my life, I believe that having a disability as a medical professional may be advantageous in being able to effectively empathise with patients suffering from other long-term health issues. With disabled people aged between 16-64 reporting lowered well-being ratings on happiness; worthwhile and life satisfaction scores; and increased anxiety levels than non-disabled counterparts, the NHS is currently failing to provide adequate support to those with continuing health problems (Office for National Statistics, 2021). Hence, as a training doctor, I recognise that I will be in a privileged position to raise awareness about the psychological burden of lasting illness among my able-bodied colleagues and the general public. In doing so, I hope that healthcare workers will begin to take a holistic approach in viewing disability and think further than treating the body and look also to healing the mind.
The introduction of the Equality Act 2010, was a positive step into protecting people with disabilities from discrimination within the workplace and wider population, demonstrating the unquestionable progression society has made in accepting disability from the brazen Victorian freak shows. Such legislation introduced by the government has had an instrumental influence in encouraging people with disabilities into employment and societal activities (i.e., sports, community groups and higher education). For example, between 2013 – 2020, there was an increase of 8.1% in the proportion of disabled people in employment, with 2.6 million disabled women and 1.8 million disabled men working, demonstrating the constructive role of such parliamentary bills (Powell, 2021). Although the apparent improvements, the uneducated reactions I witnessed towards the lamb’s defects, along with my own experiences, would suggest that even in the 21st century, disabled people are inevitably going to be made to feel unsafe by the minority who still view difference as ugly.
In conclusion, the artefact identifies and represents the exploitation of vulnerable individuals with deformities and highlights the dangerous way humans react to things that they are unfamiliar with. I observed how most of the responses to this piece within the gallery, were profoundly negative, and I have come to believe that this reaction of repugnance is reflective of the poor treatment of disabled people within today’s society. This piece has led to me uncovering the failures of the healthcare system in the past to protect individuals most at risk from mistreatment and has opened my eyes to the challenges I may encounter during my medical career in terms of counteracting negative public perception of disabilities.
Although legislation introduced by the government aims to pave the way for a more optimistic future whereby disabled people are not faced with judgment and prejudice, such discrimination is rooted within British history, and thus I appreciate it will take time to fully shift public opinion. I, therefore, hope in the future as a medical student, I can educate those around me about the damaging consequences of ignorance towards difference, and support those who face maltreatment because they do not fit into the idealistic prototype pushed by society.
Reference list-
Bahjat, M. (2018) Chang and Eng Bunker (1811-1874). Available at: https://embryo.asu.edu/pages/chang-and-eng-bunker-1811-1874 (Accessed: 13 April 2022).
Cherri, A. (2022) The Adoration of the Golden Calf, after Poussin [taxidermy] The National Gallery, London (Viewed: 11 April 2022).
Durbach, N. (2012) ‘Skin Wonders’: Body Worlds and the Victorian Freak Show’, Journal of the History of Medicine and Allied Sciences, 69(1), pp. 38-67. Available at: https://doi.org/10.1093/jhmas/jrs035
Equality Act 2010, c. 1. Available at: https://www.legislation.gov.uk/ukpga/2010/15/part/11/chapter/1 (Accessed: 13 April 2022).
Grande, L. (2010) ‘Strange and Bizarre: The History of Freak Shows’, Things said
and done. Available at: https://thingssaidanddone.wordpress.com/2010/09/26/strange-and-bizarre-the-history-of-freak-shows/ (Accessed: 12 April 2022).
Kattel, P. (2018) ‘Conjoined Twins’, Journal of Nepal Medical Association, 56(211), pp.708-710. Available at: https://www.jnma.com.np/jnma/index.php/jnma/article/view/3526/2764 (Accessed: 12 April 2022).
Leonard, T. (2014) ‘How the original Siamese twins had 21 children by two sisters… while sharing one (reinforced) bed’, The Daily Mail, 7 November. Available at: https://www.dailymail.co.uk/news/article-2825888/How-original-Siamese-twins-21-children-two-sisters-sharing-one-reinforced-bed.html (Accessed: 13 April 2022).
Martin, E. and Law, J. (eds) (2020) Concise Medical Dictionary. 10th edn. Oxford: Oxford University Press.
Office for National Statistics (2021) Outcomes for disabled people in the UK: 2020. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/disability/articles/outcomesfordisabledpeopleintheuk/2020 (Accessed: 27 April 2022).
Powell, A. (2021) Disabled people in employment. (House of Commons Library briefing paper 7540). Available at: https://researchbriefings.files.parliament.uk/documents/CBP-7540/CBP-7540.pdf (Accessed: 13 April 2022).
Wilson, C. (2011) ‘Man held after Poussin painting is vandalised at National Gallery’, The Guardian, 17 July. Available at: https://www.theguardian.com/uk/2011/jul/17/poussin-attack-national-gallery (Accessed: 12 April 2022).